
Shoulder Subluxation in Baseball: The “Diving Shoulder” Injury
Shoulder subluxations are common in baseball players who dive into bases or make diving plays in the field, particularly when the shoulder is forced into extension, abduction, and external rotation. While not a full dislocation, subluxations can still damage stabilizing structures of the shoulder, including the capsule, labrum, and rotator cuff.
Dislocation: Shoulder pops out and requires relocation by a trained professional
Subluxation: Shoulde pops out and pops back in
Early diagnosis, stabilization, and a structured return-to-throwing plan are critical to avoid recurrence and long-term instability.
What Is a Shoulder Subluxation?
A subluxation is a partial dislocation where the humeral head slips partially out of the glenoid but reduces (returns to place) spontaneously.
In baseball, this often occurs:
- When diving head-first into a base
- On a fully extended arm reaching for a ball
- From posterior or inferior force vectors (i.e., diving with arm outstretched)
This can stretch or tear:
- Glenohumeral joint capsule
- Anterior labrum
- Rotator cuff stabilizers
- Humeral head cartilage
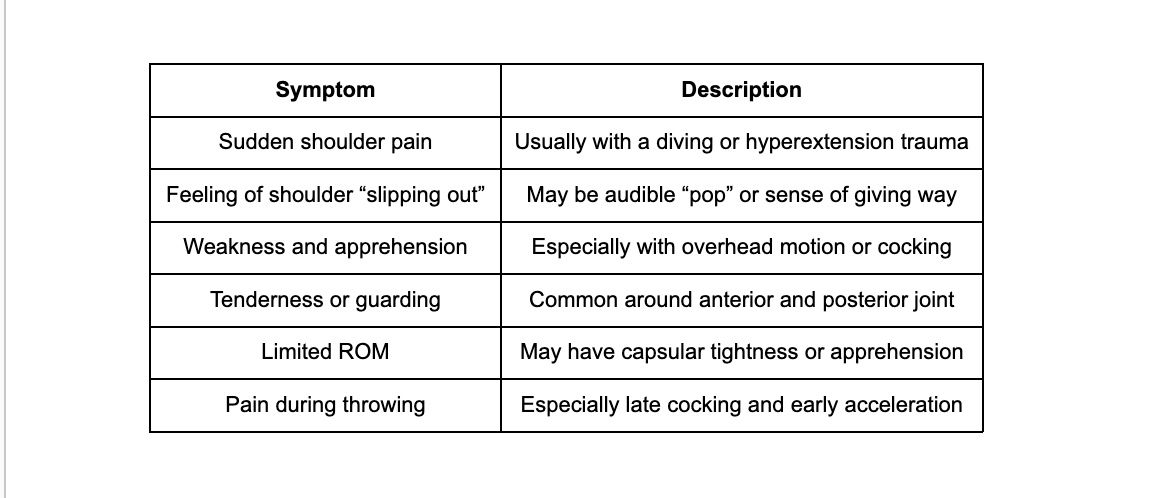
Clinical Presentation
Imaging
- X-ray: Often normal (rule out fracture or Hill-Sachs lesion)
- MRI (or MRA): Best for evaluating labral or capsular injury, especially if pain persists >2–3 weeks
Non-Operative Rehabilitation Protocol
(For athletes without gross instability or labral tear requiring surgery)
Phase 1: Acute Protection & Pain Reduction (Week 0–2)
Goals: Decrease inflammation, protect structures, begin gentle activation
- Sling for comfort (≤1 week)
- Modalities: Ice, laser therapy (6–8 J/cm²), e-stim as needed
- Submaximal isometrics: ER/IR, abduction, flexion, extension
- Scapular control drills: serratus punches, scap squeezes
- Avoid abduction + ER positions (dislocation vector)
Phase 2: Mobility & Stability (Week 2–4)
Goals: Regain ROM, begin dynamic stabilization
- PROM → AAROM → AROM
- Begin rhythmic stabilization drills (supine and seated)
- Scapular retraction and upward rotation strengthening
- Resistance band ER/IR in neutral and slight abduction
- Initiate core stability and kinetic chain integration
Phase 3: Strengthening & Neuromuscular Control (Week 4–6+)
Goals: Restore shoulder strength, overhead tolerance
- Full RTC strengthening (ER/IR, scaption, prone rows)
- Closed chain stability (wall walks, ball on wall)
- Plyometric drills: chest pass, side throws
- Begin light overhead work (modified throwing motion with towel or plyoball)
- Posterior shoulder mobility (sleeper stretch, cross-body stretch)
Phase 4: Return-to-Throwing Progression (Week 6–10+)
Goals: Return to sport-specific demands
- Initiate return-to-throwing program (see checklist below)
- Integrate core and lower body strength: med ball slams, rotational throws
- Continue shoulder endurance work (higher volume RTC, deceleration drills)
- Ensure overhead mechanics normalized and pain-free
- Position-specific drills: throwing from knees, simulated dives
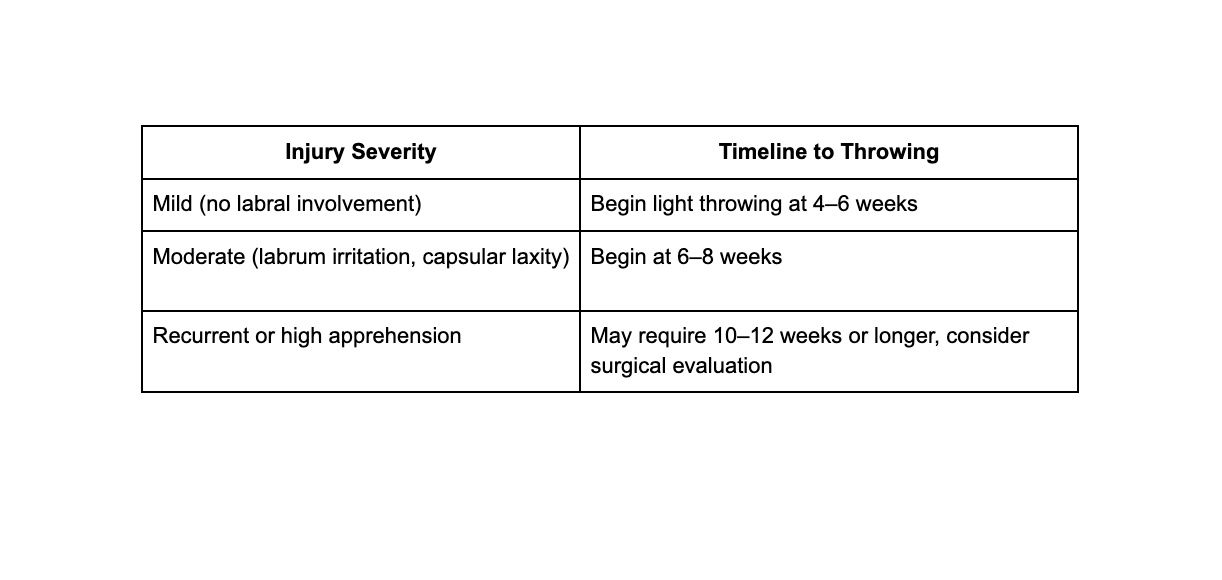
Return-to-Throwing Timeline (General Guidelines)
Return-to-Throwing Checklist
- Full, pain-free ROM (especially ER at 90°)
- 90–95% strength in rotator cuff and scapular muscles
- No apprehension with overhead or diving motion
- Successful completion of towel and plyo-ball drills
- Negative sulcus sign and anterior apprehension test
- Pain-free catch/throw progressions (short toss → long toss)
References
1. Owens BD, et al. Shoulder instability in young athletes. Am J Sports Med. 2010.
2. Wilk KE, Arrigo CA. Rehabilitation of the overhead athlete’s shoulder. Clin Sports Med. 2011.
3. Dines JS, et al. Glenohumeral instability in throwing athletes. J Bone Joint Surg Am. 2015.
4. Burkhart SS, Morgan CD. The peel-back mechanism. Arthroscopy. 2001.
5. Ellenbecker TS, et al. Rehabilitation following first-time shoulder subluxation. NSCA Performance Training Journal. 2009.